Foot Bunions Surgery
Overview
 A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
A bunion is a firm, fluid-filled pad overlying the inside of the joint at the base of the big toe (metatarsophalangeal joint). The pad (bursa), which may get larger and stick out, can become inflamed and painful. Bunions may run in families, but many result from wearing tight shoes. Nine out of 10 bunions are developed by women. Nine out of 10 women wear shoes that are too small. Tight shoes also can cause other disabling foot problems like corns, calluses and hammertoes.
Causes
You may get bunions if the way your foot is shaped puts too much pressure on your big toe joint. Because bunions can run in families, some experts believe that the inherited shape of the foot makes some people more likely to get them. Your foot rolls inward too much when you walk. A moderate amount of inward roll, or pronation, is normal. But damage and injury can happen with too much pronation. You have flat feet. You often wear shoes that are too tight. All of these may put pressure on the big toe joint. Over time, the constant pressure forces the big toe out of alignment, bending it toward the other toes.
Symptoms
The main sign of a bunion is the big toe pointing towards the other toes on the same foot, which may force the foot bone attached to it (the first metatarsal) to stick outwards. Other symptoms may include a swollen, bony bump on the outside edge of your foot, pain and swelling over your big toe joint that's made worse by pressure from wearing shoes, hard, callused and red skin caused by your big toe and second toe overlapping, sore skin over the top of the bunion, changes to the shape of your foot, making it difficult to find shoes that fit. These symptoms can sometimes get worse if the bunion is left untreated, so it's best to see a GP. They'll ask you about your symptoms and examine your foot. In some cases, an X-ray may be recommended to assess the severity of your bunion. Anyone can develop a bunion, but they're more common in women than men. This may be because of the style of footwear that women wear.
Diagnosis
A thorough medical history and physical exam by a physician is necessary for the proper diagnosis of bunions and other foot conditions. X-rays can help confirm the diagnosis by showing the bone displacement, joint swelling, and, in some cases, the overgrowth of bone that characterizes bunions. Doctors also will consider the possibility that the joint pain is caused by or complicated by Arthritis, which causes destruction of the cartilage of the joint. Gout, which causes the accumulation of uric acid crystals in the joint. Tiny fractures of a bone in the foot or stress fractures. Infection. Your doctor may order additional tests to rule out these possibilities.
Non Surgical Treatment
Bunions may be treated conservatively with changes in shoe gear, different orthotics (accommodative padding and shielding), rest, ice and medications. These sorts of treatments address symptoms more than they correct the actual deformity. Surgery, by an orthopedic surgeon or a podiatric surgeon, may be necessary if discomfort is severe enough or when correction of the deformity is desired. Orthotics are splints or regulators while conservative measures include various footwear like gelled toe spacers, bunion toes separators, bunion regulators, bunion splints and bunion cushions. There are a variety of available orthotics (or orthoses) including over-the-counter or off-the-shelf commercial products and as necessary, custom-molded orthotics that are generally prescribed medical devices. 
Surgical Treatment
If conservative treatment doesn't provide relief from your symptoms, you may need surgery. The goal of bunion surgery is to relieve discomfort by returning your toe to the correct position. There are a number of surgical procedures for bunions, and no one technique is best for every problem. Surgical procedures for bunions might involve removing the swollen tissue from around your big toe joint. Straightening your big toe by removing part of the bone. Realigning the long bone between the back part of your foot and your big toe, to straighten out the abnormal angle in your big toe joint. Joining the bones of your affected joint permanently. It's possible you may be able to walk on your foot immediately after a bunion procedure. However, full recovery can take weeks to months. To prevent a recurrence, you'll need to wear proper shoes after recovery. It's unlikely that you'll be able to wear narrower shoes after surgery. Surgery isn't recommended unless a bunion causes you frequent pain or interferes with your daily activities. Talk to your doctor about what you can expect after bunion surgery.
Prevention
There are some steps that may help prevent, or at least slow, the progression of bunions. Avoid shoes with a narrow toe box. If your foot flattens excessively, make sure you wear supportive shoes, and if necessary, get custom orthotics from your podiatrist. See your podiatrist at the first signs or symptoms of a bunion deformity, as early treatment may stop or slow its progression.
Will Overpronation Require An Operation
Overview
Over pronation of the foot is commonly referred to as "flat feet." Many middle-aged men and women suffer from over pronation over time and as a result of wearing poor-fitting shoes, continuing with repetitive exercising habits, or walking in high heels for long periods over several years. Regular speed-walkers often experience over pronation as well as a result of this activity.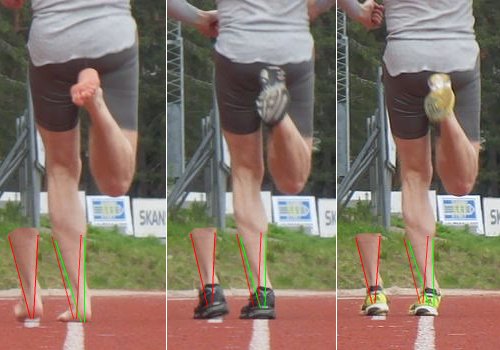
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Over pronation of the foot is commonly referred to as "flat feet." Many middle-aged men and women suffer from over pronation over time and as a result of wearing poor-fitting shoes, continuing with repetitive exercising habits, or walking in high heels for long periods over several years. Regular speed-walkers often experience over pronation as well as a result of this activity.
Causes
Although there are many factors that can contribute to the development of these conditions, improper biomechanics of the body plays a large and detrimental role in the process. Of the many biomechanical elements involved, foot and ankle function perhaps contribute the most to these aches and pains.
Symptoms
Common conditions seen with overpronation include heel pain or plantar fasciitis. Achilles tendonopathy. Hallus Valgus and/or bunions. Patellofemoral pain syndrome. Iliotibial band pain syndrome. Low back pain. Shin splints. Stress fractures in the foot or lower leg.
Diagnosis
The best way to discover whether you have a normal gait, or if you overpronate, is to visit a specialty run shop, an exercise physiologist, a podiatrist or a physical therapist who specializes in working with athletes. A professional can analyze your gait, by watching you either walk or run, preferably on a treadmill. Some facilities can videotape your gait, then analyze the movement of your feet in slow-motion. Another (and less costly) way is to look at the bottom of an older pair of run shoes. Check the wear pattern. A person with a normal gait will generally see wear evenly across the heel and front of the shoe. A person who overpronates will likely see more wear on the OUTside of the heel and more wear on the INside of the forefoot (at the ball). A person who supinates will see wear all along the outer edges of the shoe. You can also learn about your gait by looking at your arches. Look at the shape your wet feet leave on a piece of paper or a flat walking surface.
Non Surgical Treatment
If you overpronate, you should talk with a foot and ankle specialist, especially if symptoms have not developed yet. Questions you may want to ask your doctor include what are the best running shoes on the market? Where can I find those shoes? If over-the-counter orthotics don?t work, how long should I wait before contacting you for custom-made orthotics? On my next visit, what type of diagnostic testing should I expect? If I limit the amount of time I spend running, will my overpronation symptoms disappear? What additional treatment options can we try?
Prevention
Many of the prevention methods for overpronation-orthotics, for example-can be used interchangeably with treatment methods. If the overpronation is severe, you should seek medical attention from a podiatrist who can cast you for custom-made orthotics. Custom-made orthotics are more expensive, but they last longer and provide support, stability, and balance for the entire foot. You can also talk with a shoe specialist about running shoes that offer extra medial support and firm heel counters. Proper shoes can improve symptoms quickly and prevent them from recurring. Surgery can sometimes help cure and prevent this problem if you suffer from inherited or acquired pes planus deformity. Surgery typically involves stabilizing the bones to improve the foot?s support and function.
Calcaneal Apophysitis The Truth
Overview
The true name of this complaint is calcaneal apophysitis which just means an inflamation of the growth centre of the bone in your heel as a result of pulling by the Achilles tendon - it is important to realise that it is not a disease but rather a condition that develops in the growing skeleton with activity. It is the most common cause of heel pain in young athletes, and is the second most common condition of its kind in the younger athelete after Osgood-Schlatter's disease. It is often seen at a time of rapid growth during which the muscles and soft tissues become tighter as the bones get longer. It occurs more in boys than girls and is seen most commonly between the ages of 8 and 14 years though it tends to be more prevalent in the younger of this group.
Causes
Sever's disease can result from standing too long, which puts constant pressure on the heel. Poor-fitting shoes can contribute to the condition by not providing enough support or padding for the feet or by rubbing against the back of the heel. Although Sever's disease can occur in any child, these conditions increase the chances of it happening. Pronated foot (a foot that rolls in at the ankle when walking), which causes tightness and twisting of the Achilles tendon, thus increasing its pull on the heel's growth plate. Flat or high arch, which affects the angle of the heel within the foot, causing tightness and shortening of the Achilles tendon. Short leg syndrome (one leg is shorter than the other), which causes the foot on the short leg to bend downward to reach the ground, pulling on the Achilles tendon. Overweight or obesity, which puts weight-related pressure on the growth plate.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, worsening of pain after exercise, a tender swelling or bulge on the heel that is sore to touch, calf muscle stiffness first thing in the morning, limping, a tendency to tiptoe.
Diagnosis
A Podiatrist can easily evaluate your child?s foot, lower limbs and muscular flexibility, to identify if a problem exists. If a problem is identified, a simple treatment plan is put in place. Initial treatment may involve using temporary padding and strapping to control motion or to cushion the painful area and based on the success of this treatment, a long-term treatment plan will be put in place. This long-term treatment plan may or may not involve Foot Supports, Heel Raises, muscle stretching and or strengthening.
Non Surgical Treatment
If your child lets you know that his heels are hurting, schedule a doctor's appointment. Your family doctor may or may not refer you to a podiatrist. Treatment for Sever's Disease typically consists of one or more of the following steps. Reducing physical activity. Because Sever's Disease appears to be most common in athletic children, reducing exercise periods will relieve pressure on the heel bones, thereby reducing pain. Your doctor may recommend that your child take a complete break from athletic activity for a set amount of time. Icing the heel bones can help to lower both inflammation and pain levels. Use a cold pack or wrap ice in a towel and apply it to the heels. A new exercise regimen that involves simple stretches designed to lengthen the calf muscles and tendons. Your doctor may prescribe the use of orthotic shoe inserts that will assist your child in maintaining a good level of physical activity. HTP Heel Seats may be an excellent option and have been purchased by many parents as an effective aide for children suffering from Sever's Disease. Read about HTP Heel Seats here and ask your doctor if they are right for your child's unique case. In extreme cases, a doctor may recommend a plaster cast or boot, but typically only if other less cumbersome solutions fail to reduce pain. Some doctors may prescribe anti-inflammatory medications. Never give these to a child yourself, without first seeking a doctor's advice. Some medications carry the risk of serious side effects for children. Only give medications if specifically prescribed your child's physician.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
The true name of this complaint is calcaneal apophysitis which just means an inflamation of the growth centre of the bone in your heel as a result of pulling by the Achilles tendon - it is important to realise that it is not a disease but rather a condition that develops in the growing skeleton with activity. It is the most common cause of heel pain in young athletes, and is the second most common condition of its kind in the younger athelete after Osgood-Schlatter's disease. It is often seen at a time of rapid growth during which the muscles and soft tissues become tighter as the bones get longer. It occurs more in boys than girls and is seen most commonly between the ages of 8 and 14 years though it tends to be more prevalent in the younger of this group.
Causes
Sever's disease can result from standing too long, which puts constant pressure on the heel. Poor-fitting shoes can contribute to the condition by not providing enough support or padding for the feet or by rubbing against the back of the heel. Although Sever's disease can occur in any child, these conditions increase the chances of it happening. Pronated foot (a foot that rolls in at the ankle when walking), which causes tightness and twisting of the Achilles tendon, thus increasing its pull on the heel's growth plate. Flat or high arch, which affects the angle of the heel within the foot, causing tightness and shortening of the Achilles tendon. Short leg syndrome (one leg is shorter than the other), which causes the foot on the short leg to bend downward to reach the ground, pulling on the Achilles tendon. Overweight or obesity, which puts weight-related pressure on the growth plate.
Symptoms
A few signs and symptoms point to Sever?s disease, which may affect one or both heels. These include pain at the heel or around the Achilles tendon, Heel pain during physical exercise, especially activities that require running or jumping, worsening of pain after exercise, a tender swelling or bulge on the heel that is sore to touch, calf muscle stiffness first thing in the morning, limping, a tendency to tiptoe.
Diagnosis
A Podiatrist can easily evaluate your child?s foot, lower limbs and muscular flexibility, to identify if a problem exists. If a problem is identified, a simple treatment plan is put in place. Initial treatment may involve using temporary padding and strapping to control motion or to cushion the painful area and based on the success of this treatment, a long-term treatment plan will be put in place. This long-term treatment plan may or may not involve Foot Supports, Heel Raises, muscle stretching and or strengthening.
Non Surgical Treatment
If your child lets you know that his heels are hurting, schedule a doctor's appointment. Your family doctor may or may not refer you to a podiatrist. Treatment for Sever's Disease typically consists of one or more of the following steps. Reducing physical activity. Because Sever's Disease appears to be most common in athletic children, reducing exercise periods will relieve pressure on the heel bones, thereby reducing pain. Your doctor may recommend that your child take a complete break from athletic activity for a set amount of time. Icing the heel bones can help to lower both inflammation and pain levels. Use a cold pack or wrap ice in a towel and apply it to the heels. A new exercise regimen that involves simple stretches designed to lengthen the calf muscles and tendons. Your doctor may prescribe the use of orthotic shoe inserts that will assist your child in maintaining a good level of physical activity. HTP Heel Seats may be an excellent option and have been purchased by many parents as an effective aide for children suffering from Sever's Disease. Read about HTP Heel Seats here and ask your doctor if they are right for your child's unique case. In extreme cases, a doctor may recommend a plaster cast or boot, but typically only if other less cumbersome solutions fail to reduce pain. Some doctors may prescribe anti-inflammatory medications. Never give these to a child yourself, without first seeking a doctor's advice. Some medications carry the risk of serious side effects for children. Only give medications if specifically prescribed your child's physician.
Recovery
If the child has a pronated foot, a flat or high arch, or another condition that increases the risk of Sever's disease, the doctor might recommend special shoe inserts, called orthotic devices, such as heel pads that cushion the heel as it strikes the ground, heel lifts that reduce strain on the Achilles tendon by raising the heel, arch supports that hold the heel in an ideal position. If a child is overweight or obese, the doctor will probably also recommend weight loss to decrease pressure on the heel. The risk of recurrence goes away on its own when foot growth is complete and the growth plate has fused to the rest of the heel bone, usually around age 15.
What Are The Signs And Symptoms Of A Ruptured Achilles Tendon?
Overview
 When a tendon ruptures it can be extremely painful and cause a disability of the foot that then subsequently causes damage to the ankle joints. The tendons in the ankle include: the peroneals (peroneus brevis, peroneus longus,) anterior tibialis, posterior tibialis, and Achilles tendon. Any of these structures can become ruptured, which is a serious condition that will typically require surgery to fix.
When a tendon ruptures it can be extremely painful and cause a disability of the foot that then subsequently causes damage to the ankle joints. The tendons in the ankle include: the peroneals (peroneus brevis, peroneus longus,) anterior tibialis, posterior tibialis, and Achilles tendon. Any of these structures can become ruptured, which is a serious condition that will typically require surgery to fix.
Causes
There are a number of factors that can increase the risk of an Achilles tendon rupture, which include the following. You?re most likely to rupture your Achilles tendon during sports that involve bursts of jumping, pivoting and running, such as football or tennis. Your Achilles tendon becomes less flexible and less able to absorb repeated stresses, for example of running, as you get older. Small tears can develop in the fibres of the tendon and it may eventually completely tear. There is a very small risk of an Achilles tendon rupture if you have Achilles tendinopathy (also called Achilles tendinitis). This is where your tendon breaks down, which causes pain and stiffness in your Achilles tendon, both when you exercise and afterwards. If you take quinolone antibiotics and corticosteroid medicines, it can increase your risk of an Achilles tendon injury, particularly if you take them together. The exact reasons for this aren't fully understood at present.
Symptoms
If your Achilles tendon is ruptured you will experience severe pain in the back of your leg, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound is heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone.
Diagnosis
During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if it has ruptured completely. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order an ultrasound or MRI scan. These painless procedures create images of the tissues of your body.
Non Surgical Treatment
There is no definitive protocol for conservative management. Traditionally, conservative treatment involved immobilisation in a cast or boot, with initial non-weight bearing. Recently, good results have been achieved with functional bracing and early mobilisation, and it is common to be immediately weight-bearing in an orthotic. Conservative management reduces the chance of complications, such as infection. There is a risk the tendon can heal too long and more slowly. 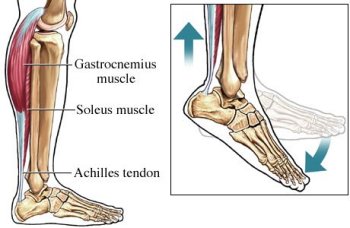
Surgical Treatment
Thanks to a new surgical technique, operative procedures are often more beneficial.The operative treatment of Achilles tendon ruptures has significantly changed in recent years. The objective today is to connect the torn tendons using modern suture and possibly adhesive materials. Through small surgical incisions the ends of the torn tendon are surgically exposed, and sutures are used to tie the ends permanently together. Thus, the operated repaired tendon is again resilient within a reasonable time. The cast treatment and walking on crutches required in the past, is with this procedure usually not necessary. Instead, functional treatment following the surgery involves wearing a special boot, meaning that the patient can put weight onto the operated leg again within a few days after surgery. Physical therapy training will start immediately following the operation. The philosophy behind such an early functional treatment is that tissue adequately adapts to stress and thus accelerates the healing process. For the patient, the modern surgical treatment of an Achilles tendon rupture has the distinct advantage that no prolonged hospital stay is necessary. Hospital stay usually lasts only a few days. Using crutches, patients can return to work soon after the surgery.
Leg Length Discrepancy Treatment In Adults
Overview
Many people don?t realise it, but one of their legs is longer (or shorter) than the other one. Over time, this can lead to degenerative osteoarthritis (OA) in the hip joint requiring a hip replacement. But the surgeon can?t just take the old hip joint out and put the new implant in. Careful planning, special surgical techniques, and adjusting of the implant component parts are important in preventing continuation or even worsening of the leg length discrepancy.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.

Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Many people don?t realise it, but one of their legs is longer (or shorter) than the other one. Over time, this can lead to degenerative osteoarthritis (OA) in the hip joint requiring a hip replacement. But the surgeon can?t just take the old hip joint out and put the new implant in. Careful planning, special surgical techniques, and adjusting of the implant component parts are important in preventing continuation or even worsening of the leg length discrepancy.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.
Surgical Treatment
Your child will be given general anesthetic. We cut the bone and insert metal pins above and below the cut. A metal frame is attached to the pins to support the leg. Over weeks and months, the metal device is adjusted to gradually pull the bone apart to create space between the ends of the bones. New bone forms to fill in the space, extending the length of the bone. Once the lengthening process is completed and the bones have healed, your child will require one more short operation to remove the lengthening device. We will see your child regularly to monitor the leg and adjust the metal lengthening device. We may also refer your child to a physical therapist to ensure that he or she stays mobile and has full range of motion in the leg. Typically, it takes a month of healing for every centimeter that the leg is lengthened.
Posterior Tibial Tendon Insufficiency Treatment
Overview
Originally known as posterior tibial tendon dysfunction or insufficiency, adult-acquired flatfoot deformity encompasses a wide range of deformities. These deformities vary in location, severity, and rate of progression. Establishing a diagnosis as early as possible is one of the most important factors in treatment. Prompt early, aggressive nonsurgical management is important. A patient in whom such treatment fails should strongly consider surgical correction to avoid worsening of the deformity. In all four stages of deformity, the goal of surgery is to achieve proper alignment and maintain as much flexibility as possible in the foot and ankle complex. However, controversy remains as to how to manage flexible deformities, especially those that are severe. 
Causes
Causes of an adult acquired flatfoot may include Neuropathic foot (Charcot foot) secondary to Diabetes mellitus, Leprosy, Profound peripheral neuritis of any cause. Degenerative changes in the ankle, talonavicular or tarsometatarsal joints, or both, secondary to Inflammatory arthropathy, Osteoarthropathy, Fractures, Acquired flatfoot resulting from loss of the supporting structures of the medial longitudinal arch. Dysfunction of the tibialis posterior tendon Tear of the spring (calcaneoanvicular) ligament (rare). Tibialis anterior rupture (rare). Painful flatfoot can have other causes, such as tarsal coalition, but as such a patient will not present with a change in the shape of the foot these are not included here.
Symptoms
Symptoms shift around a bit, depending on what stage of PTTD you?re in. For instance, you?re likely to start off with tendonitis, or inflammation of the posterior tibial tendon. This will make the area around the inside of your ankle and possibly into your arch swollen, reddened, warm to the touch, and painful. Inflammation may actually last throughout the stages of PTTD. The ankle will also begin to roll towards the inside of the foot (pronate), your heel may tilt, and you may experience some pain in your leg (e.g. shin splints). As the condition progresses, the toes and foot begin to turn outward, so that when you look at your foot from the back (or have a friend look for you, because-hey-that can be kind of a difficult maneuver to pull off) more toes than usual will be visible on the outside (i.e. the side with the pinky toe). At this stage, the foot?s still going to be flexible, although it will likely have flattened somewhat due to the lack of support from the posterior tibial tendon. You may also find it difficult to stand on your toes. Finally, you may reach a stage in which your feet are inflexibly flat. At this point, you may experience pain below your ankle on the outside of your foot, and you might even develop arthritis in the ankle.
Diagnosis
It is of great importance to have a full evaluation, by a foot and ankle specialist with expertise in addressing complex flatfoot deformities. No two flat feet are alike; therefore, "Universal" treatment plans do not exist for the Adult Flatfoot. It is important to have a custom treatment plan that is tailored to your specific foot. That starts by first understanding all the intricacies of your foot, through an extensive evaluation. X-rays of the foot and ankle are standard, and MRI may be used to better assess the quality of the PT Tendon.
Non surgical Treatment
Non-surgical treatment includes rest and reducing your activity until the pain improves. Orthotics or bracing help support the tendon to reduce its pull along the arch, thus reducing pain. In moderate to severe cases, a below knee cast or walking boot may be needed to allow the tendon to rest completely and heal. Physical therapy is an integral part of the non-surgical treatment regimen to reduce inflammation and pain. Anti-inflammatory medication is often used as well. Many times evaluation of your current shoes is necessary to ensure you are wearing appropriate shoe gear to prevent re-injury. 
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
Posterior Tibial Tendon Dysfunction (PTTD) Treatment And Cause
Overview Most flat feet are not painful, particularly those flat feet seen in children. In the adult acquired flatfoot, pain occurs because soft tissues (tendons and ligaments) have been torn. The deformity progresses or worsens because once the vital ligaments and posterior tibial tendon are lost, nothing can take their place to hold up the arch of the foot. The painful, progressive adult acquired flatfoot affects women four times as frequently as men. It occurs in middle to older age people with a mean age of 60 years. Most people who develop the condition already have flat feet. A change occurs in one foot where the arch begins to flatten more than before, with pain and swelling developing on the inside of the ankle. Why this event occurs in some people (female more than male) and only in one foot remains poorly understood. Contributing factors increasing the risk of adult acquired flatfoot are diabetes, hypertension, and obesity.  Causes Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder. Symptoms Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain. Diagnosis Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered. Non surgical Treatment Orthotic or anklebrace, Over-the-counter or custom shoe inserts to position the foot and relieve pain are the most common non-surgical treatment option. Custom orthotics are often suggested if the shape change of the foot is more severe. An ankle brace (either over-the-counter or custom made) is another option that will help to ease tendon tension and pain. Boot immobilization. A walking boot supports the tendon and allows it to heal. Activity modifications. Depending on what we find, we may recommend limiting high-impact activities, such as running, jumping or court sports, or switching out high-impact activities for low-impact options for a period of time. Ice and anti-inflammatory medications. These may be given as needed to decrease your symptoms.
Causes Posterior tibial tendon dysfunction is the most common cause of acquired adult flatfoot deformity. There is often no specific event that starts the problem, such as a sudden tendon injury. More commonly, the tendon becomes injured from cumulative wear and tear. Posterior tibial tendon dysfunction occurs more commonly in patients who already have a flat foot for other reasons. As the arch flattens, more stress is placed on the posterior tibial tendon and also on the ligaments on the inside of the foot and ankle. The result is a progressive disorder. Symptoms Patients will usually describe their initial symptoms as "ankle pain", as the PT Tendon becomes painful around the inside of the ankle joint. The pain will become more intense as the foot flattens out, due to the continued stretching and tearing of the PT Tendon. As the arches continue to fall, and pronation increases, the heel bone (Calcaneus) tilts into a position where it pinches against the ankle bone (Fibula), causing pain on both the inside and outside of the ankle. As the foot spends increased time in a flattened, or deformed position, Arthritis can begin to affect the joints of the foot, causing additional pain. Diagnosis Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered. Non surgical Treatment Orthotic or anklebrace, Over-the-counter or custom shoe inserts to position the foot and relieve pain are the most common non-surgical treatment option. Custom orthotics are often suggested if the shape change of the foot is more severe. An ankle brace (either over-the-counter or custom made) is another option that will help to ease tendon tension and pain. Boot immobilization. A walking boot supports the tendon and allows it to heal. Activity modifications. Depending on what we find, we may recommend limiting high-impact activities, such as running, jumping or court sports, or switching out high-impact activities for low-impact options for a period of time. Ice and anti-inflammatory medications. These may be given as needed to decrease your symptoms.  Surgical Treatment Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.
Surgical Treatment Stage two deformities are less responsive to conservative therapies that can be effective in mild deformities. Bone procedures are necessary at this stage in order to recreate the arch and stabilize the foot. These procedures include isolated fusion procedures, bone grafts, and/or the repositioning of bones through cuts called osteotomies. The realigned bones are generally held in place with screws, pins, plates, or staples while the bone heals. A tendon transfer may or may not be utilized depending on the condition of the posterior tibial tendon. Stage three deformities are better treated with surgical correction, in healthy patients. Patients that are unable to tolerate surgery or the prolonged healing period are better served with either arch supports known as orthotics or bracing such as the Richie Brace. Surgical correction at this stage usually requires fusion procedures such as a triple or double arthrodesis. This involves fusing the two or three major bones in the back of the foot together with screws or pins. The most common joints fused together are the subtalar joint, talonavicular joint, and the calcaneocuboid joint. By fusing the bones together the surgeon is able to correct structural deformity and alleviate arthritic pain. Tendon transfer procedures are usually not beneficial at this stage. Stage four deformities are treated similarly but with the addition of fusing the ankle joint.